A man with the disease
link
to picture
A man with the disease
link
to picture
The bacteria Clostridium tetani is the cause
of the disease called tetanus, or Lockjaw. The occurrence of tetanus
in the United States is rather low, because of the widespread use of tetanus
immunizations. However, the bacteria does accounts for several hundred
thousand infant deaths around the world each year. Just a cup of
the toxin that this bacteria produces could possibly kill all the humans
on the plant (2).
Clostridium tetani
Clostridium tetani is a Gram positive bacilli.
It can form spores, a differentiated, specialized cell that is used
by an organism for survival in times of adverse
conditions. These spores are resistant to heat and chemical agents.
It takes autoclaving or boiling Clostridium tetani for at least four hours
before it is completely
killed. It is an obligate anaerobe, which means that it is killed
in the presence of oxygen (1), for this reason it can not be established
in a human tissue unless it is at
the site of a wound which is poorly supplied with blood (2).
Outside of the human body, Clostridium tetani, can
be found in many places. In nature, it is readily found in soil as
well as the gastrointestinal tracts of animals
such as: horses, sheep, cattle, dogs, cats, and chickens (1).
Infection is cause by accidental puncture wounds,
burns, umbilical stumps, frostbite, and crushed body parts (2). Infants
usually get the antibody from their
mothers transpacentally, however if the mother has never been vaccinated,
neonatal tetanus can occur. It is usually associated with nonsterile
delivery and/or
improper umbilical cord care (3).
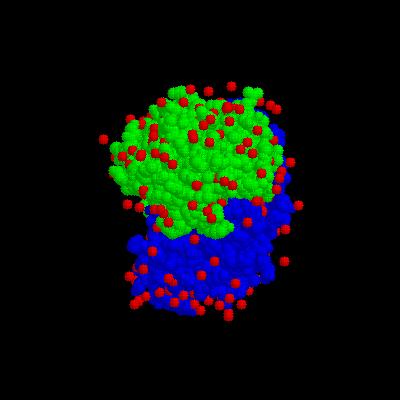
What happens at the molecular level
The toxin Tetanospasmin is the known cause of the
problems associated with the disease tetanus. The protein has a 30%
to 40% homology to botulinum toxins,
the cause of common food poisoning (1). It has one heavy chain
that has a molecular weight of 100 kDa as well as a light chain of 50 kDa.
These subunits are
linked together by a disulfide bond.
The light chain has a tetrahedral zinc binding motif,
which includes two histidines, a glutamate, and a water molecule.
The heavy chain is marked with a carboxyl terminal, it has a immunogenic,
a neuronal cell binding and ganglioside binding site, as well as a retrograde
transport (1).
The bacteria enters the body at the site of the wound.
The toxin spreads to the nearby motor nerve endings, and travels by axons
to the ventral horns of the
spinal cord (2). When in the spinal cord, the toxin binds to
the membrane and is taken up by endocytosis. This transport across
the membrane is mediated by the
tetanus heavy chain. The N-terminal of the heavy chain forms
a pore. The light chain of the toxin is then free to move to the
inhibitory presynaptic terminal of the
motor neuron. From here the toxin moves from the vesicle to cytosol,
intracellular fluid. This movement is facilitated by a low pH which
is found in the vesicle.
When in the proper cell the toxin affects the release
of inhibitory transmitters, glycine or GABA, by cleaving the synaptobrevin.
This cleavage occurs at
glutamate 76 (1).
Symptoms
The incubation period is from three to twenty-one
days, shorter incubation is associated with more contamination of the wound
(4). After the toxin has reached
its target, it affects the ability of the body to control muscle contractions.
Powerful muscle contractions result, starting with the jaw moving down
the body (2).
These intense muscle spasms may last seconds to minutes. Not
only are these contractions painful, but many times they are forceful enough
to break bones,
especially the vertebrae. Death is most often a result of the
paralysis of respiratory muscles and respiratory collapse (2). The
disease is at its worst for four to
fourteen days, with complete recovery over many months (1). After
full recovery, no permanent damage to the muscles usually remains (2).
The onset of tetanus is
associated 30-90% fatality rate, higher in the neonatal type and in
the elderly.
The neonatal type of tetanus is common in developing
areas. It is caused by unhygienic child birth practices like smearing
cow dung or ghee (clarified butter) on
the umbilical stump. It begins five to fifteen days after birth
and is marked by poor sucking and excessive crying (1).
Treatment
Tetanus is uncommon in industrial areas, but it is
more common in underdeveloped areas, especially agricultural area (4).
This is largely due to the fact that
although tetanus is one of the worlds most preventable diseases by
vaccination, this vaccine is not available in all areas (2). Another
problem with the immunization
is over 90% of patients never complete the series. With the full
immunization, a person is protected from the disease 100%. The recommended
vaccination series
starts with one to three month old infants, and consist of three injections
given two months apart. A booster dose is given about one to four
years later, then every
ten years after (2).
Antibody responses and/or organisms at the site of
infection are rare, so a person thought to have the disease must be monitored
for symptoms (4). During one
of the muscle spasms a spatula test may be down to see if it is in
fact tetanus. For this test a spatula is inserted into the pharynx,
if the person does have tetanus
they will bite the spatula, if the test is negative, he or she will
gag and expel the spatula (1). After it is determined that a patient
has tetanus, the free toxin needs to
be neutralized. This is done by administering human Tetanus immune
globulin (TIG) (1). If TIG is not available, tetanus antitoxin should
be used (4). The problem
with the tetanus antitoxin is it comes from horses, an allergic reaction
may occur and should be monitored (2).
The antitoxin
link
to picture
Respiratory support and actions against metabolic
complications must be taken into account, as well as controlling the muscle
spasms. To control muscle
contractions, anti-spasm drugs, or even neuromuscular blocking agents
may be necessary. Tetanus is also susceptible to Penicillin G, Erythromycin,
and
Tetracycline (1).